MultiMed Engineers conducted a cost-effectiveness analysis for assessing the frailty prevention scheme based on the City4Age Project’s early detection system.
Available evidence for conducting the analysis is linked to the longitudinal observational studies conducted in the frame of the City4Age Pilot experiments (in particular, the one carried out in the city of Athens), which enabled us to train and measure the performance of a classifier for robustness in elderly citizens – one of the central elements of the Project’s early detection approach.
Since such evidence alone is not enough to feed and run an HTA model, additional information has been derived from the scientific literature. For this, we mostly relied on the extensive knowledge and references provided by the EU-supported Joint Action ADVANTAGE.
The analysis was conducted with the support of the MAFEIP Framework, which has been developed to support evidence-based decision-making processes for all institutions and users in the health and care sector, in particular in the frame of the EIP on AHA initiative.
The analysis is based on a three-state Markov model, as represented in the following Figure.
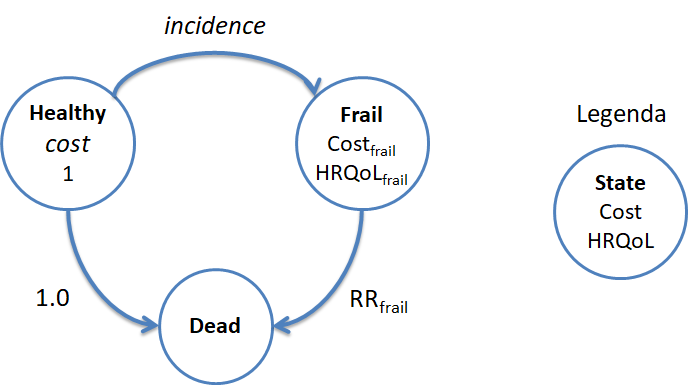
Figure 1. Markov model for conducting the City4Age HTA
The analysis has been first conducted from the perspective of the Public Health Authorities, in order to assess how the City4Age approach might improve Health Related Quality of Life (HRQoL) in elderly populations, while at the same time shifting resource usage from expensive healthcare settings, typically sustained by public health systems, to a more efficient wellbeing self-management context, sustained by the private sector.
After populating the model’s parameters and running it on the MAFEIP Tool, the following Incremental Cost-Effectiveness Ration (ICER) has been obtained.
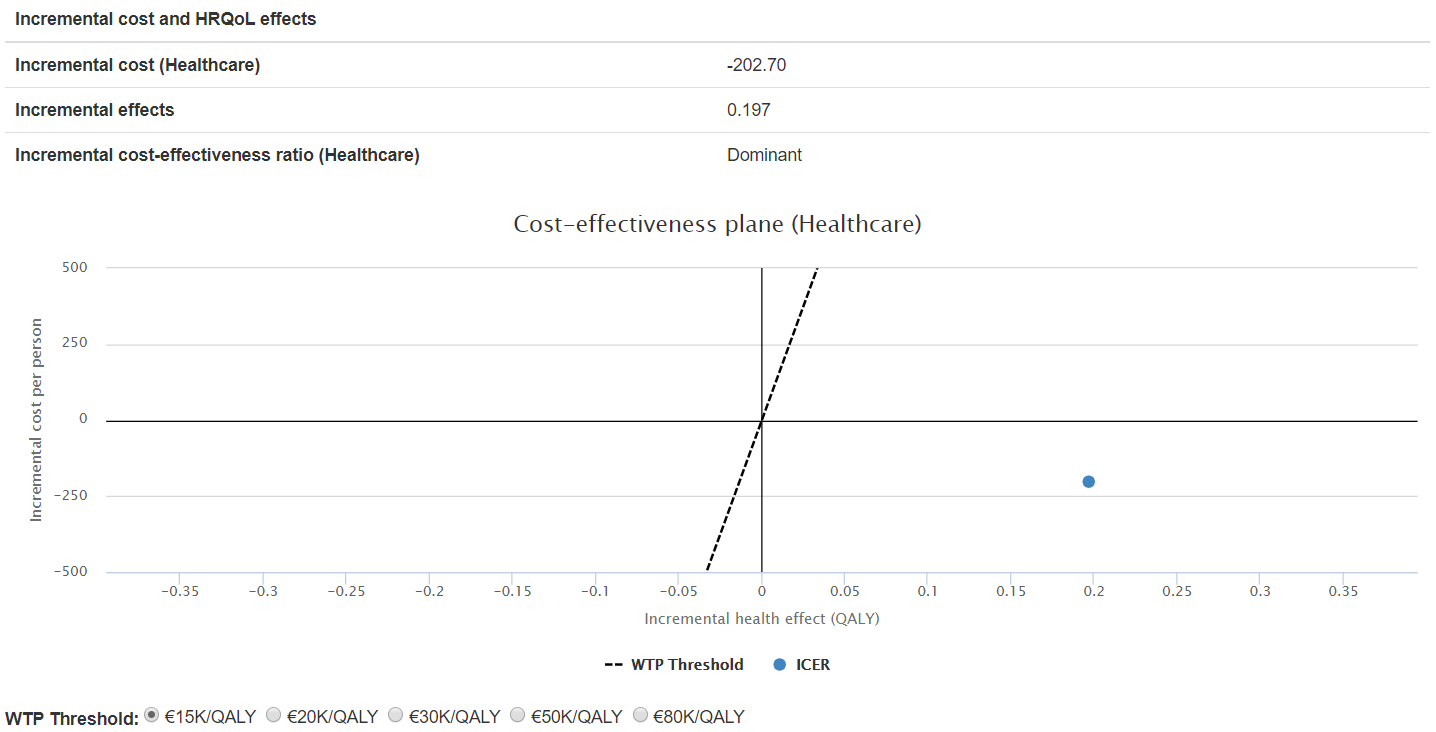
Figure 2. ICER for the City4Age early detection system, Healthcare perspective
The ICER location shows that the City4Age solution dominates the current standard of care, and it is thus viable from the Healthcare point of view, allowing Public HC Systems to gain almost 0.2 QALYs per patient, while saving at the same time 200 € per patient.
Since this strategy rests in part on shifting costs from cure to prevention, the latter being paid by citizens themselves, it is important to consider the effect of this shift on the ICER, in order to verify that the system is not uneconomic from the overall societal point of view.
The following Figure shows the results of this check.
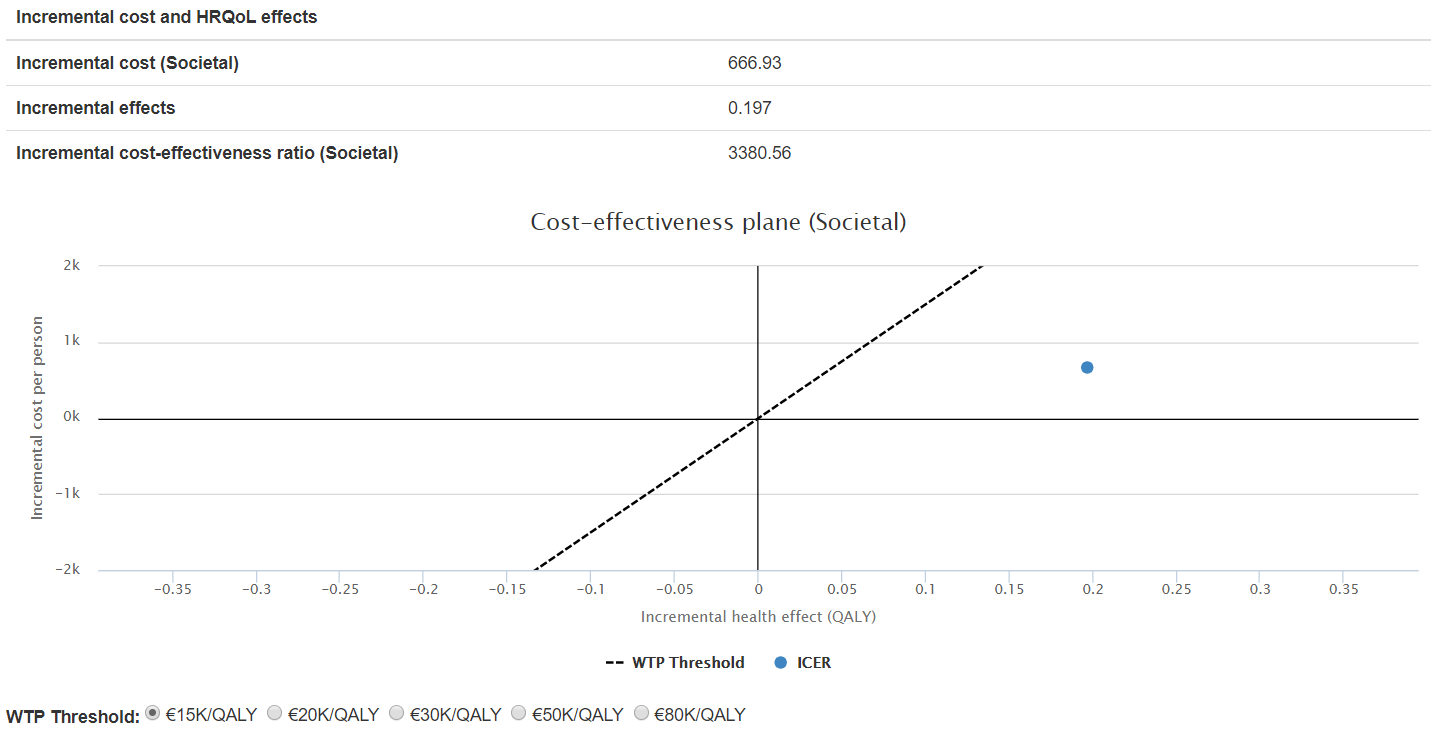
Figure 3. ICER for the City4Age early detection system, Societal perspective
With respect to the Healthcare perspective, presented in Figure 2, the City4Age solution is not dominant in this case. However, at 3,380 €/QALY, it is still confirmed as highly cost effective and viable even at the lowest Willingness-To-Pay thresholds.
Limitations
The most important limitation of this analysis is that, not being based on an RCT with a proper control arm, we had to rely extensively on “secondary” literature data, not always fully consistent with our objectives.
In particular, we feel that the most important weakness is that we were not able to express gender-specific scenarios, given the demonstrated difference in frailty epidemiology among sexes (worse in females vs males)[1]. To solve this issue, more studies would be necessary to fill the current gap in available data (e.g. to assess gender-specific incidence rates, gender-specific relative risks of mortality, etc.).
The full report of the City4Age HTA is available as a Case Study on the MAFEIP Portal.
[1] Gordon et al. Sex differences in frailty: A systematic review and meta-analysis, Exp Gerontol. 2017